




SUMMARY
-
Developmental Dysplasia of the Hip is a disorder of abnormal development resulting in dysplasia, subluxation, and possible dislocation of the hip secondary to capsular laxity and mechanical instability.
-
Diagnosis can be confirmed with ultrasonography in the first 4 months and then with radiographs after femoral head ossification occurs (~ 4-6 months).
-
Treatment varies from Pavlik bracing to surgical reduction and osteotomies depending on the age of the patient, underlying etiology, and the severity of dysplasia.
EPIDEMIOLOGY
-
Incidence
-
most common orthopaedic disorder in newborns
-
dysplasia is 1:100
-
dislocation is 1:1000
-
-
Demographics
-
more common in females (6:1)
-
more commonly seen in Native Americans and Laplanders
-
due to cultural traditions such as swaddling with hips together in extension
-
-
rarely seen in African Americans
-
-
Anatomic location
-
most common in left hip (60%)
-
due to the most common intrauterine position being left occiput anterior (left hip is adducted against the mother's lumbrosacral spine)
-
-
bilateral in 20%
-
-
Risk factors
-
firstborn
-
due to unstretched uterus and tight abdominal structures compressing the uterus
-
-
female
-
due to increased ligamentous laxity that transiently exists as the result of circulating maternal hormones and the estrogens produced by the fetal uterus
-
-
breech
-
more commonly seen in female children, firstborn children, and pregnancies complicated by oligohydramnios
-
higher risk of DDH with frank/single breech position compared to footling breech position
-
-
family history
-
oligohydramnios
-
macrosomia
-
limited hip abduction
-
talipes
-
swaddling
-
ETIOLOGY
-
DDH encompasses a spectrum of disease that includes
-
dysplasia
-
shallow or underdeveloped acetabulum
-
-
subluxation
-
displacement of the joint with some contact remaining between the articular surfaces
-
-
dislocation
-
complete displacement of the joint with no contact between the original articular surfaces
-
-
teratologic hip
-
dislocated in utero and irreducible on neonatal exam
-
presents with a pseudoacetabulum
-
associated with neuromuscular conditions and genetic disorders
-
commonly seen with arthrogryposis, myelomeningocele, Larsen's syndrome, Ehlers-Danlos
-
-
late (adolescent) dysplasia
-
mechanically stable and reduced but dysplastic
-
-
-
Pathophysiology
-
etiology
-
initial instability thought to be caused by maternal and fetal laxity, genetic laxity, and intrauterine and postnatal malpositioning
-
-
pathoanatomy
-
initial instability leads to dysplasia
-
typical deficiency is anterior or anterolateral acetabulum
- in spastic cerebral palsy, acetabular deficiency is posterosuperior
- in spastic cerebral palsy, acetabular deficiency is posterosuperior
-
-
dysplasia leads to subluxation and gradual dislocation
-
repetitive subluxation of the femoral head leads to the formation of a ridge of thickened articular cartilage called the limbus
-
-
chronic dislocation leads to
-
development of secondary barriers to reduction
-
pulvinar thickens
-
ligamentum teres thickens and elongates
-
transverse acetabular ligament hypertrophies
-
hip capsule and iliopsoas form hourgass configuration
-
-
anatomic changes
-
increased femoral anteversion
-
flattening of the femoral head
-
increased acetabular anteversion
-
increased obliquity and decreased concavity of the acetabular roof
-
thickening of the medial acetabular wall
-
-
-
-
-
Associated conditions
-
associated with "packaging" deformities which include
-
congenital muscular torticollis (20%)
-
metatarsus adductus (10%)
-
congenital knee dislocation
-
-
conditions characterized by increased amounts of type III collagen
-
CLASSIFICATION
-
Can be classified as a spectrum of disease involvement (phases)
-
subluxable
-
Barlow-suggestive
-
-
dislocatable
-
Barlow-positive
-
-
dislocated
-
Ortolani-positive early when reducible; Ortolani-negative late when irreducible
-
-
PRESENTATION
-
Physical exam (< 3 months)
- mainstay of physical diagnosis is palpable hip subluxation/dislocation on exam
-
Barlow
-
dislocates a dislocatable hip by adduction and depression of the flexed femur
-
"click of exit"
-
- Ortolani
-
reduces a dislocated hip by elevation and abduction of the flexed femur
-
"click of entry"
-
-
Galeazzi (Allis)
-
apparent limb length discrepancy due to a unilateral dislocated hip with hip flexed at 90 degrees and feet on the table
-
femur appears shortened on dislocated side
-
-
-
hip clicks are nonspecific findings
-
Barlow and Ortolani are rarely positive after 3 months of age because of soft-tissue contractures that form around the hip
- mainstay of physical diagnosis is palpable hip subluxation/dislocation on exam
-
Physical exam (> 3 months to 1 year)
- limitations in hip abduction
-
most sensitive test once contractures have begun to occur
-
occurs as laxity resolves and stiffness begins to occur
-
decreased symmetrically in bilateral dislocations
-
-
leg length discrepancy predominates
-
Klisic test
-
used to detect bilateral dislocations
-
line from the long finger placed over the greater trochanter and the index finger over the ASIS should point to the umbilicus
-
if the hip is dislocated, the line will point halfway between the umbilicus and pubis
-
- limitations in hip abduction
-
Physical exam (> 1 year - walking child)
-
pelvic obliquity
-
lumbar lordosis
-
in response to hip contractures resulting from bilateral dislocations in a child of walking age
-
-
Trendelenburg gait
-
results from abductor insufficiency
-
-
toe-walking
-
attempt to compensate for the relative shortening of the affected side
-
-
IMAGING
-
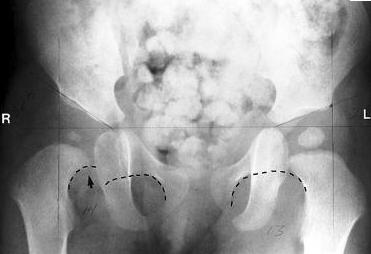
Radiograph
-
indications
- becomes primary imaging modality at 4-6 mo after the femoral head begins to ossify
-
positive physical exam
-
leg length discrepancy
- becomes primary imaging modality at 4-6 mo after the femoral head begins to ossify
-
recommended views
-
AP of pelvis
-
- measurements
-
hip dislocation
-
Hilgenreiner's line
-
horizontal line through the right and left triradiate cartilage
-
femoral head ossification should be inferior to this line
-
- Perkin's line
-
line perpendicular to Hilgenreiner's line through a point at the lateral margin of the acetabulum
-
femoral head ossification should be medial to this line
-
- Shenton's line
-
arc along the inferior border of the femoral neck and the superior margin of the obturator foramen
-
arc line should be continuous
-
-
delayed ossification of the femoral head is seen in cases of dislocation
- acetabular teardrop not typically present prior to hip reduction for chronic dislocations since birth
-
development of teardrop after reduction is thought to be a good prognostic sign for hip function
-
-
-
hip dysplasia
-
acetabular index (AI)
-
angle formed by Hilgenreiner's line and a line from a point on the lateral triradiate cartilage to a point on lateral margin of acetabulum
- should be < 25° in patients older than 6 months
-
-
center-edge angle (CEA) of Wiberg
-
angle formed by Perkin's line and a line from the center of the femoral head to the lateral edge of the acetabulum
-
< 20° is considered abnormal
-
only reliable in patients > 5 years old
-
-
-
-
-
Ultrasound
-
indications
-
primary imaging modality from birth to 4 months
-
may produce spurious results if performed before 4-6 weeks of age
-
-
positive physical exam
-
risk factors (family history or breech presentation)
-
AAP recommends an US study at 6 weeks in patients who are considered high risk (family history or breech presentation) despite normal exam
-
- monitoring of reduction during Pavlik harness treatment
-
most studies show it is not cost effective for routine screening
-
-
findings
-
evaluates for acetabular dysplasia and/or the presence of a hip dislocation
- allows view of bony acetabular anatomy, femoral head, labrum, ligamentum teres, hip capsule
-
normal ultrasound in patients with soft-tissue clicks will have normal acetabular development
-
-
measurements
- alpha angle
-
angle created by lines along the bony acetabulum and the ilium
-
normal is > 60°
-
-
beta angle
-
angle created by lines along the labrum and the ilium
-
normal is < 55°
-
-
femoral head is normally bisected by a line drawn down from the ilium
- alpha angle
-
staging
- Graf classification
-
Arthrogram
-
indications
-
used to confirm reduction after closed reduction under anesthesia
-
- help identify possible blocks to reduction
-
inverted labrum
-
labrum enhances the depth of the acetabulum by 20% to 50% and contributesto the growth of the acetabular rim
-
in the older infant with DDH, the labrum may be inverted and may mechanically block concentric reduction of the hip
-
-
inverted limbus
-
represents a pathologic response of the acetabulum to abnormal pressures caused by superior migration of the femoral head
-
consists of fibrous tissue
-
-
transverse acetabular ligament
-
located at the caudal perimeter of the acetabulum
-
in persistent hip dislocation, becomes contracted and can act as a block to reduction
-
- hip capsule is constricted by iliopsoas tendon causing hourglass deformity of the capsule
-
pulvinar
-
fibrofatty tissue within the acetabulum that can act as a block to reduction
-
spontaneously regresses after the hip is reduced
-
-
ligamentum teres
-
acts as minor source of blood supply to femoral head
-
in persistent hip dislocation, it lengthens and hypertrophies and can act as a block to reduction
-
-
-
-
CT
- historically the study of choice to evaluate reduction of the hip after closed reduction and spica casting
- historically the study of choice to evaluate reduction of the hip after closed reduction and spica casting
-
MRI
-
increasingly used to evaluate reduction of hip after closed reduction and spica casting in order to minimize radiation compared to CT
-
-
-
Arthrogram
-
indications
-
used to confirm reduction after closed reduction under anesthesia
-
- help identify possible blocks to reduction
-
inverted labrum
-
labrum enhances the depth of the acetabulum by 20% to 50% and contributesto the growth of the acetabular rim
-
in the older infant with DDH, the labrum may be inverted and may mechanically block concentric reduction of the hip
-
-
inverted limbus
-
represents a pathologic response of the acetabulum to abnormal pressures caused by superior migration of the femoral head
-
consists of fibrous tissue
-
-
transverse acetabular ligament
-
located at the caudal perimeter of the acetabulum
-
in persistent hip dislocation, becomes contracted and can act as a block to reduction
-
- hip capsule is constricted by iliopsoas tendon causing hourglass deformity of the capsule
-
pulvinar
-
fibrofatty tissue within the acetabulum that can act as a block to reduction
-
spontaneously regresses after the hip is reduced
-
-
ligamentum teres
-
acts as minor source of blood supply to femoral head
-
in persistent hip dislocation, it lengthens and hypertrophies and can act as a block to reduction
-
-
-
-
CT
- historically the study of choice to evaluate reduction of the hip after closed reduction and spica casting
- historically the study of choice to evaluate reduction of the hip after closed reduction and spica casting
-
MRI
-
increasingly used to evaluate reduction of hip after closed reduction and spica casting in order to minimize radiation compared to CT
-
SCREENING
-
All infants require screening
-
physical exam
-
successful screening requires repetitive screening until walking age
-
-
ultrasound
-
ultrasound screening of all infants occurs in many countries; however, it has not been proven to be cost-effective
-
USA recommendation is to perform ultrasound at 4-6 weeks in patients with
-
risk factors
-
positive physical findings
-
- AAP recommends an US study at 6 weeks in patients who are considered high risk (family history or breech presentation) despite normal exam
-
also utilized to follow Pavlik treatment or for equivocal exams
-
-
TREATMENT IN CHILDREN
-
Non-operative
- abduction splinting/bracing (Pavlik harness)
-
indications
-
< 6 months old and reducible hip
-
-
contraindicated in teratologic hip dislocations and patients with spina bifida or spasticity
-
requires normal muscle function for successful outcomes
-
-
-
closed reduction and spica casting
-
indications
-
6-18 months old
-
failure of Pavlik treatment
-
-
- abduction splinting/bracing (Pavlik harness)
-
Operative
-
open reduction and spica casting
-
indications
-
> 18 months old
-
failure of closed reduction
-
-
- open reduction and femoral osteotomy
-
indications
- > 2 years old with residual hip dysplasia
-
anatomic changes on femoral side (e.g., femoral anteversion, coxa valga)
-
best in younger children (< 4 years old)
-
after 4 years old, pelvic osteotomies are utilized
-
- > 2 years old with residual hip dysplasia
-
-
open reduction and pelvic osteotomy
-
indications
-
> 2 years old with residual hip dysplasia
- severe dysplasia accompanied by significant radiographic changes on the acetabular side (increased acetabular index)
-
used more commonly in older children (> 4 yr)
-
decreased potential for acetabular remodeling as child ages
-
-
-
-
TECHNIQUES
-
Abduction splinting/bracing (Pavlik harness)
-
goals
-
treatment is based on an early concentric reduction in order to prevent future degeneration of the hip
-
risk, complexity, and complications are increased with delays in diagnosis
-
-
technique
-
positioning
-
anterior straps flex the hips to 90-100° flexion and prevent extension
-
posterior straps prevent adduction of the hips
-
-
confirm position with ultrasound or radiograph and monitor every 4-6 weeks
-
worn for 23 hours/day for at least 6 weeks or until hip is stable
-
wean out of harness over 6-8 weeks after hip has stabilized until normal anatomy develops
-
discontinue if hip is not reduced by 3-4 weeks to prevent Pavlik disease
-
-
complications specific to this treatment
-
AVN
-
due to impingement of the posterosuperior retinacular branch of the medial femoral circumflex artery
-
seen with extreme abduction (> 60°)
-
prevent via placement of abduction within safe zone
-
zone located between the angle of maximal passive hip abduction and the angle of hip adduction at which the femoral head displaces from the acetabulum when the hips are in 90° of flexion
-
-
-
transient femoral nerve palsy
-
seen with hyperflexion
-
-
Pavlik disease
-
erosion of the pelvis superior to the acetabulum and prevention of the development of the posterior wall of the acetabulum due to prolonged positioning of dislocated hip in flexion and abduction
-
important to discontinue the harness if the hip is not reduced by 3-4 weeks
-
-
-
outcomes
-
overall success rate of 90%
-
dependent upon age at initiation of treatment and time spent in the harness
-
- abandon Pavlik harness treatment if not successful after 3-4 weeks
-
If Pavlik harness fails, consider converting to semi-rigid abduction brace with weekly ultrasounds for an addition 3-4 weeks before considering further intervention
-
-
-
Closed reduction and spica casting
-
anesthesia
-
performed under general anesthesia
-
excessive force can result in AVN
-
-
-
technique
-
closed reduction
-
reduce using the Ortolani maneuver (hip flexion and abduction while elevating the greater trochanter)
-
-
arthrogram
-
used to confirm the reduction
-
must obtain concentric reduction with < 5mm of contrast pooling medial to femoral head and no interposition of the limbus
- medial dye pool > 7mm associated with poor outcomes and AVN
- medial dye pool > 7mm associated with poor outcomes and AVN
-
also helps identify anatomic blocks to reduction
-
-
adductor tenotomy
-
perform if the patient has an unstable safe zone (i.e. if excessive abduction is required to maintain the reduction)
-
-
spica casting
-
immobilize in 100° of hip flexion and 45° of abduction with neutral rotation for 3 months
-
"human position"
-
wide abduction associated with AVN (aim for < 55° abduction)
-
- confirm reduction with CT scan in spica cast with selective cuts to minimize radiation to the child
-
change cast at 6 weeks
-
-
-
complications specific to this treatment
-
AVN
-
risk factors
-
extreme abduction > 60°
-
due to impingement of the posterosuperior retinacular branch of the medial femoral circumflex artery
-
prevent via placement of abduction within safe zone
-
zone located between the angle of maximal passive hip abduction and the angle of hip adduction at which the femoral head displaces from the acetabulum when the hips are in 90° of flexion
-
-
-
medial dye pool > 7mm
-
indicates unstable reduction
-
-
-
-
-
-
Open reduction
-
approach
-
anterior approach (Smith-Peterson)
-
most commonly used due to decreased risk of injury to the medial femoral circumflex artery
-
capsulorrhaphy can be performed after reduction
-
used if the patient is > 12 months old
-
-
medial approach
-
pros
-
directly addresses block to reduction
-
can be used in patients < 12 months old
-
decreased blood loss
-
-
cons
-
unable to perform a capsulorrhaphy
-
higher risk of AVN
-
-
types
-
Ludloff
-
medial approach
-
performed between the pectineus and adductor longus and brevis
-
-
Weinstein
-
anteromedial approach
- performed between neurovascular bundle and pectineus
-
-
Ferguson
-
posteromedial approach
-
performed superficially between the adductor longus and gracilis, and deep between the adductor brevis and adductor magnus
-
-
-
-
-
soft tissue
-
remove possible anatomic blocks to reduction
-
iliopsoas contracture, capsular constriction, inverted labrum, pulvinar, hypertrophied ligamentum teres
-
-
perform adductor tenotomy if the patient has an unstable safe zone (i.e. if excessive abduction is required to maintain the reduction)
-
-
post-op
-
immobilize in functional position of 30° of flexion, 30° of abduction and 30° of internal rotation
-
-
-
Femoral Varus DeRotational Osteotomy (VDRO)
-
indications
-
femoral shortening
-
facilitates reduction
-
decreases the risk of AVN by relieving the tension produced by the reduction of a previously dislocated hip
-
-
correct excessive femoral anteversion and/or valgus
-
-
used after femoral head is congruently reduced with satisfactory ROM and reasonable femoral sphericity
-
- Pelvic Osteotomies
-
indications
-
increase anterior or anterolateral coverage
- increased acetabular index consistent with acetabular dysplasia
-
-
used after reduction is confirmed on abduction-internal rotation views and satisfactory ROM has been obtained
-
COMPLICATIONS
-
AVN
-
seen with all forms of treatment
-
increased rates associated with
-
excessive or forceful abduction
-
previous failed closed treatment
-
repeat surgery
-
-
diagnosis based on radiographic findings that include
-
failure of appearance or growth of the ossific nucleus 1 year after the reduction
-
broadening of the femoral neck
-
increased density and fragmentation of ossified femoral head
-
residual deformity of proximal femur after ossification
-
-
-
Delayed diagnosis
-
bilateral dislocations
-
patients typically function better if hips are not reduced if 6 years of age or older
-
-
unilateral dislocation
-
better outcomes without surgical treatment if the patient is > 8 years old
-
epiphysiodesis can be performed for treatment of limb length discrepancy
-
-
-
Recurrence
-
approximately 10% with appropriate treatment
-
requires radiographic follow-up until skeletal maturity
-
-
Transient femoral nerve palsy
-
seen with excessive flexion during Pavlik bracing
-