 Orthopedic emergency
Orthopedic emergency



SUMMARY
-
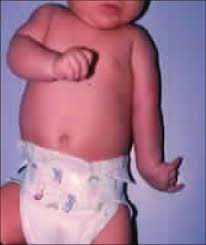
Obstetric Brachial Plexopathy is injury to the brachial plexus that occurs during birth usually as a result of a stretching injury from a difficult vaginal delivery.
-
Diagnosis is made clinically and depends on the nerve roots involved.
-
Treatment can be observation or operative depending on the nerve roots involved, the severity of injury, and the location of the nerve injury.
EPIDEMIOLOGY
-
Incidence
-
approximately 1 to 4 per 1,000 live births
-
decreasing in frequency due to improved obstetric care
-
-
Anatomic location
-
often right sided or bilateral
-
- Risk factors
-
large for gestational age (macrosomia)
-
multiparous pregnancy
-
difficult presentation
-
shoulder dystocia
-
forceps delivery
-
breech position
-
prolonged labor
-
ETIOLOGY
-
Cause
-
usually a stretching injury from a difficult vaginal delivery
-
some rare cases reported following C-sections
-
-
Associated orthopedic conditions
- glenohumeral dysplasia
- increased glenoid retroversion, humeral head flattening, posterior humeral head subluxation
-
develops in 70% of infants with obstetric brachial plexopathy
-
caused by Internal rotation contracture (loss of external rotation)
-
- increased glenoid retroversion, humeral head flattening, posterior humeral head subluxation
-
elbow flexion contracture
-
etiology is unclear, likely due to persistent relative triceps weakness (C7) compared with biceps (C5-6)
-
-
clavicle and humerus fractures
-
torticollis
- glenohumeral dysplasia
ANATOMY
-
Brachial plexus diagram
-
-
Narakas Classification
-
Group
-
Characteristics
-
Roots
-
Group I (Duchenne-Erb's Palsy)
-
Paralysis of deltoid and biceps.
-
Intact wrist and digital flexion/extension.
-
C5-C6
-
Group II (Intermediate Paralysis)
-
Paralysis of deltoid, biceps, and wrist and digital extension.
-
Intact wrist and digital flexion.
-
C5-C7
-
Group III (Total Brachial Plexus Palsy)
-
Flail extremity without Horner's syndrome
-
C5-T1
-
Group IV (Total Brachial Plexus Palsy with Horner's syndrome)
-
Flail extremity with Horner's syndrome
-
C5-T1
-
-
Waters Classification of Glenohumeral Deformity
-
-
Waters Classification of Glenohumeral Deformity
-
Classification
-
Radiographic features
-
Type I
-
< 5 degree difference in retroversion
-
Type II
-
> 5 degree difference in retroversion
-
Type III
-
Posterior humeral head subluxation
-
< 35% anterior to scapular spine axis
-
Type IV
-
Presence of false glenoid
-
Type V
-
Flattening of humeral head, progressive/ complete humeral head dislocation
-
Type VI
-
Infantile posterior dislocation
-
Type VII
-
Proximal humeral growth arrest
-
PRESENTATION GENERAL
-
Symptoms
-
lack of active hand and arm motion
-
-
Physical exam
-
upper extremity exam
-
arm hangs limp at side in an adducted and internally rotated position
-
decreased shoulder external rotation
-
affected shoulder subluxates posteriorly
-
-
provocative testing
-
stimulate neonatal reflexes including Moro, asymmetric tonic neck and Vojta reflexes
-
pain with gentle shaking of a flail arm may indicate pseudoparalysis from infection or fracture rather than nerve palsy
-
-
Hospital for Sick Children Active Movement Scale (AMS) muscle strength grading system
-
full range of motion with gravity eliminated (score of 4) must be achieved before higher scores may be assigned
-
-
IMAGING
-
Radiographs
-
may be useful for evaluation of clavicle or humerus fractures
-
limited utility in infant given minimal ossification of humeral head and glenoid
-
axillary view to evaluate position of humeral head if patient is older and suspicion is high for joint subluxation
-
-
Myelography/CT myelography/MRI
-
may be used to distinguish between root avulsion and extraforaminal rupture
-
-
EMG/NCV
-
poor reliability and often underestimate the severity of injury
-
-
Ultrasound
-
allows for assessment of joint subluxation or dislocation
-
ERB'S PALSY (C5,6) - UPPER LESION
- Most common type
-
Mechanism
-
results from lateral flexion of the head towards the contralateral shoulder with depression of the ipsilateral shoulder producing traction on plexus
-
occurs during difficult delivery in infants
-
-
-
Physical exam
-
adducted, internally rotated shoulder; pronated forearm, extended elbow (“waiter’s tip”)
-
C5 deficiency
-
axilllary nerve deficiency
-
deltoid, teres minor weakness
-
-
suprascapular nerve deficiency
-
supraspinatus, infraspinatus weakness
-
-
musculocutaneous nerve deficiency
- biceps and brachialis weakness
- biceps and brachialis weakness
-
-
C6 deficiency
-
radial nerve deficiency
-
brachioradialis, supinator weakness
-
-
-
-
Prognosis
-
best prognosis for spontaneous recovery
-
KLUMPKE'S PALSY (C8,T1) - LOWER LESION
-
Mechanism
-
rare in obstetric palsy
-
usually arm presentation with subsequent traction/abduction from trunk
-
-
Physical exam
-
deficit of all of the small muscles of the hand (ulnar and median nerves)
-
“claw hand”
-
wrist in extreme extension because of the unopposed wrist extensors
-
hyperextension of MCP due to loss of hand intrinsics
-
flexion of IP joints due to loss of hand intrinsics
-
-
-
Prognosis
-
poor prognosis for spontaneous recovery
-
frequently associated with a preganglionic injury and Horner's Syndrome
-
TOTAL PLEXUS PALSY (C5-T1)
-
Mechanism
-
stretch, rupture, and avulsion injury
-
-
Physical exam
-
flaccid arm
-
both motor and sensory deficits
-
-
Imaging
-
chest radiograph to look for ipsilateral hemidiaphragm paralysis from phrenic nerve injury
-
-
Prognosis
-
worst prognosis
-
TREATMENT - GENERAL
-
Nonoperative
-
observation & daily passive exercises by parents
-
indications
- first line of treatment for all obstetric brachial plexopathies while awaiting return of function
- first line of treatment for all obstetric brachial plexopathies while awaiting return of function
-
key to treatment is maintaining passive motion while waiting for nerve function to return
-
-
-
Operative
- microsurgical nerve grafting
-
indications
-
lack of antigravity biceps function between 3-9 months of age
-
postganglionic injury with intact nerve roots with segmental injury to nerve
-
-
outcomes
-
improved outcomes are seen with shorter grafts (<10cm)
-
-
-
nerve transfer or neurotization
-
definition
-
nerve transfer refers to fascicles from one nerve transferred into a nother nerve that supplies a muscle
-
neurotization refers to placing nerve fascicles directly into a neuromuscular junction of a muscle
-
-
indications
-
lack of antigravity biceps function between 3-9 months of age
-
preganglionic injury or avulsion of nerve roots
-
-
- microsurgical nerve grafting
TREATMENT - SHOULDER DISLOCATION & CONTRACTURES
-
Operative
-
soft tissue procedures
- latissimus dorsi and teres major transfer (Hoffer procedure)
-
indication
-
persistent internal rotation contracture or external rotation weakness without glenohumeral dysplasia
-
-
technique
-
pass tendons posteriorly around humerus to create external rotation forces
-
-
-
pectoralis major and +/- subscapularis lengthening
-
indication
-
to lessen the internal rotation forces
-
-
may be used in conjunction with tendon transfers
-
-
arthroscopic release for internal rotation contractures
- latissimus dorsi and teres major transfer (Hoffer procedure)
-
bony procedures
- proximal humeral derotation osteotomy (Wickstrom)
-
indication
-
persistent internal rotation contracture or external rotation weakness with glenohumeral dysplasia
-
-
-
arthrodesis
-
indication
-
non-functional deltoid with good function of hand and wrist
-
-
- proximal humeral derotation osteotomy (Wickstrom)
-
TREATMENT - ELBOW FLEXION CONTRACTURE
-
Nonoperative
- serial nighttime elbow extension splinting
-
indications
-
for elbow flexion contracture <40 degrees
-
-
outcomes
-
prevents progression, does not correct contracture
-
-
-
serial elbow extension casting
-
indications
-
for elbow flexion contracture >40 degrees
-
-
- serial nighttime elbow extension splinting
-
Operative
-
anterior capsular release, biceps/brachialis tendon lengthening
-
indications
-
for severe, persistent contracture
-
-
outcomes
-
may have high recurrence rate
-
-
-
TREATMENT - FOREARM
-
Operative
-
indications
-
residual supination contracture of the forearm
-
-
technique
-
biceps rerouting tendon transfer
-
intact passive passive pronation
-
-
Operative
-
indications
-
replace function for a paralyzed muscle
-
-
force is preportional to cross-sectional area of the muscle
-
amplitude is proportional to the length of the muscle
-
technique
-
tendon transfers
-
wrist drop
-
pronator teres to ECRB
-
-
loss of finger extension
-
FCR or FCU to EDC 2-5
-
-
thumb abduction
-
EIP to abductor pollicis brevis
-
-
-
-
-
-
TREATMENT - WRIST AND HAND
-
Operative
-
indications
-
replace function for a paralyzed muscle
-
-
force is preportional to cross-sectional area of the muscle
-
amplitude is proportional to the length of the muscle
-
technique
-
tendon transfers
-
wrist drop
-
pronator teres to ECRB
-
-
loss of finger extension
-
FCR or FCU to EDC 2-5
-
-
thumb abduction
-
EIP to abductor pollicis brevis
-
-
-
-
COMPLICATIONS
-
Initial nerve inury
-
phrenic nerve palsy
-
if persistent may require diaphragm plication
-
-
-
Surgical complications
-
shoulder tendon transfers
-
radial and axillary nerve palsies
-
-
-
Phrenic nerve palsy
-
if persist may require diaphragm plication
-